








This site is for informational purposes only. Please consult with a qualified medical professional before making any dietary changes.
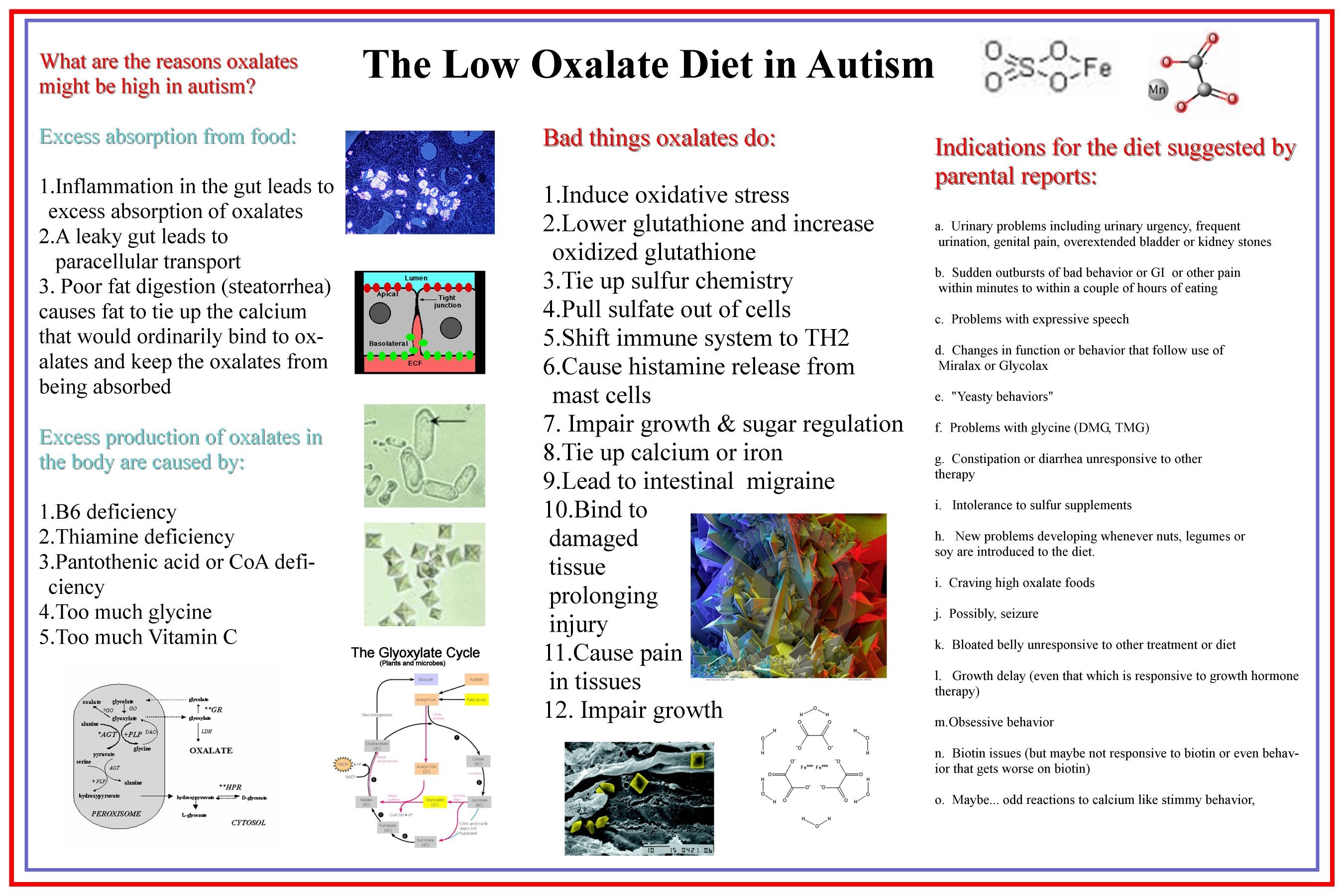
Oxalate is a highly reactive molecule that is abundant in many plant foods, but in human cells, when it is present in high amounts, it can lead to oxidative damage, depletion of glutathione, the igniting of the immune system's inflammatory cascade, and the formation of crystals which seem to be associated with pain and prolonged injury. Ordinarily, not much oxalate is absorbed from the diet, but the level of absorption has to do with the condition of the gut. There is a lot of medical literature showing that when the gut is inflamed, when there is poor fat digestion (steatorrhea), when there is a leaky gut, or when there is prolonged diarrhea or constipation, excess oxalate from foods that are eaten can be absorbed from the GI tract and become a risk to other cells in the body.
Those with a history of heavy antibiotic use or recent antibiotic use may be at much greater risk from dietary oxalate. Many antibiotics can kill back the flora that degrades oxalate, including lactobacillus acidophilus and bifidus. These bacteria that comprise the main ingredients in most probiotics may have been taken with the idea they would discourage yeast. It is a very good idea to try and replenish these familiar commensal bacterias , but they are just so-so at degrading oxalate because they really prefer other foods. That is not the case with another bacteria, which is an anaerobe called oxalobacter formigenes. Oxalobacter cannot survive without eating up oxalate, so oxalate makes it happy and makes it grow.. Several studies have shown that those who develop oxalate-related disease generally lack oxalobacter in their stool.
People who do well on a high oxalate diet may be people who have a healthy amount of oxalobacter in their colon. They might be able to eat nut breads and spinach on SCD or high-oxalate dairy substitutes on gf/cf and flours that may be high oxalate like buckwheat, because the oxalobacter would happily degrade the oxalate and keep the dietary oxalate from being absorbed in the colon where it could travel by blood into other tissues. If this is the case, a patient should have low plasma and low urinary oxalate while they are eating a high oxalate diet.
The urinary test by itself may not be sufficient for this "ruling" in populations known to have sulfation problems because insufficient sulfate inside of kidney tubule cells would be predicted to affect the ability of the kidneys to remove oxalate from the blood and deliver that oxalate to urine. This caveat regarding urinary testing would be a concern for those with autism and those with HIV, a disease known to be associated with urinary wasting of sulfate. So, a high level of oxalate in urine should be a concern, but a low level in urine may not properly represent the amount of oxalate absorbed from the gut.
The article Oxalobacter formigenesand Its Potential Role in Human Health found that many antibiotics can and do kill this special microbe called oxalobacter formigenes:
We are glad that a company named Oxthera is busy getting approval for a probiotic of oxalobacter formigenes that will be sold as a drug. It is being developed at this site: Oxthera Products.
Women in the Vulvar Pain Foundation have described a no-win scenario that may happen in other populations. They found that they were being treated prophylactically with antibiotics when they went to the doctor complaining of symptoms that suggested they had a urinary tract infection. Later, the culture would come back negative after they had already been on yet another round of antibiotics. Of course, those antibiotics may have further damaged the flora by killing off the oxalate degraders. IF OXALATE WAS THE CAUSE OF THE SYMPTOMS, then you can see that this scenario would keep the problem perpetuating itself. Many of these women found that on the low oxalate diet, they lost the symptoms that felt like a UTI, and stopped being on this antibiotic merry-go-round. Many found similar relief from yeast infections on this diet, so they no longer required constant anti-fungal medication. Clearly, this is an area where a correct diagnosis that recognizes oxalate's role in these symptoms may be able to end the otherwise endless rounds of medication...that is, IF oxalates were the cause of symptoms.
It is likely the tie to yeast infections involves a problem in the immune system and its ability to recognize yeast overgrowth and respond. Oxalate is known to impair carboxylase enzymes producing symptoms equivalent to biotin or biotinidase deficiency. The literature on those conditions is clear that when carbxylases are impaired, it is easy to get runaway problems with yeast. Perhaps this explains why some people on the low oxalate diet would lose this inhibition, resulting in a loss of their tendency towards chronic candidiasis. If this reduction of yeast doesn't seem to be working in the first months of LOD when "dumping cycles" may come more frequently, then it certainly might make sense to increase the level of biotin in the diet (with a supplement that furnishes biotin in mgs rather than mcgs) to see if that also helps keep back yeast by enhancing carboxylase activity. For a more thorough explanation of biotin-dependent enzymes and processes that we now realize may suffer inhibition by oxalate see page.309-310 in the Defeat Autism Now! manual and search the archives for biotin at Trying_Low_Oxalates.
The Defeat Autism Now! manual, though written for autism, still contains many principles that could be applied to other conditions where there may be oxidative stress, difficulty clearing toxins, gut inflammation and dysbiosis, and problems with immunity, so it is recommended as a potential resource for those with oxalate-related issues.
The Autism Oxalate Project was begun in early 2005, started by Autism Researcher Susan Costen Owens, a graduate of Vanderbilt University and the University of Texas at Dallas and long-term member of the Defeat Autism Now! Thinktank run by the Autism Research Institute. She began this project after many years of studying how the sulfate, the sulfur and the oxalate chemistries work together in our bodies and after realizing that the gut inflammation in autism characterized first by Dr. Andrew Wakefield and later by many other gastroenterologists may lead to the excess absorption of oxalate from the diet because of increased permeability. Since gastrointestinal conditions are found frequently in autism, it seemed reasonable to see if lowering the dietary supply of oxalates could be beneficial.
From inception, this project has been focused on learning from three main sources: the welcomed advice and new work produced by the finest oxalate scientists in the world who were met primarily at international conferences; from the outstanding work on oxalates represented in the medical literature; and from the amazing and ground-breaking observations of parents and other individuals using this diet who discuss their progress on the Yahoo! Group list Trying_Low_Oxalates. The potent ideas and wealth of research continue to guide our choices about which dietary supplements and other strategies are likely to maximize the improvements and minimize the down side of any periods of increased symptoms.
We quickly learned that people who had been eating a very high oxalate diet before getting on the low oxalate diet may experience a temporary worsening of autistic symptoms that we think represents oxalates leaving cells where they were sequestered before and having biological effects. This process of oxalate release has been described in genetic hyperoxalurias where the source of the oxalate was metabolic rather than from the diet, but the process is likely to be the same. On the far side of these periods that we've started to call "dumping", improvements were noted to occur in the genetic hyperoxalurias. In our project with children with autism, we also began to see improvements that involved symptoms associated with autism. Those changes included the resolution of bowel problems that had not responded to previous therapy, and introduced the concept that the bowel itself might have injury prolonged by exposure to oxalate. Our project also was pleased to find improvements occurring in gross and fine motor skills, in speech and in growth, in stimming, and in many other areas commonly seen in autism.
We have learned recently that there is common regulation between the sulfur chemistry and oxalates. You may have heard that years ago Dr. Rimland was involved with inspiring or conducting many studies that found that vitamin B6 was very effective in decreasing autistic symptoms. We now know that Vitamin B6 (pyridoxine) is a necessary cofactor for enzymes that help prevent the formation of oxalates, but this vitamin, when deficient, will also wreak havock with the sulfur chemistry in many places along the sulfur pathway. We have also learned that when sulfur is deficient, it becomes extremely difficult to keep the body from making excess oxalates. We certainly have to consider that problems in the sulfur chemistry may be why oxalates produce symtpoms in autism that are not seen in the genetic hyperoxalurias.
Before starting a low oxalate diet for an individual with autism, please take the time to fill out the ATEC form. If possible, please repeat this process every three months to chart progress. When repeating the ATEC, please do not score during a "dumping cycle".
Presentation on Oxalate in Autism from AutismOne 2007
One of the surprises that have occurred in listmates on Trying Low Oxalates using the low oxalate diet has involved changes in congestion or the condition of the lungs. Some have found that during "dumping" (when we presume that oxalates are clearing tissues) these individuals have described worsened issues with congestion. In one listmate, this even involved a hospitalization for bronchitis followed by the appearance of a kidney stone. This lady's doctors probably knew of no medical precedent for determining if oxalate clearance was involved in the onset of this temporary lung condition. The listmate reported, however, that during the period of time she was in the hospital, her temperature also fell to 35 degrees Centigrade (which is 95 Fahrenheit). This lowering of temperature may be related to issues that are discussed in our thyroid section and might possibly be related to an effect of oxalate.
Lung issues became a special interest of our listserve when listmates who had chronic congestion before the diet found that after many months, the diet helped to clear their lungs to the point that chronic congestion is no longer a problem.
We have also noticed that those with lung-related "dumping" symptoms do not appear to be the same group as those who have urinary or bowel-related "dumping" symptoms. This would make sense if there were organ specific regulation of WHERE oxalates are secreted under various biochemical persuasion. Possibly, polymorphisms in some regulatory molecules or other environmental changes could select one mode of secretion over another. There is much to learn about what accounts for differences in response to the low oxalate diet or exposure to oxalates in general.
There is not a huge corpus of literature on the lungs and oxalate except for quite a bit of discussion about how Aspergillus infections in the lungs may produce dangerous amounts of oxalate that may end up affecting other organs in the body. Even so, there is one group in Russia that has found that there could be a strong connection between chronic obstructive pulmonary disease and asthma and elevated oxalates.in lung tissues (referenced below). This work needs to be reproduced in the English speaking world to raise its visibility and to provoke an interest in doing research in this area.
Because we see lung issues in some LOD dieters during "dumping", a laboratory needs to study the possibility that the lungs, like the kidneys and the intestines and the skin, are a site of oxalate secretion from the body. Could oxalates have anything to do with the changes that take place in mucous during infection, making the mucous more painful (sore throats) or might oxalate affect how much mucous is produced with certain infections? Could the known impairment of glycolysis and the TCA cycle by oxalate be causing depletions of energy that may lead to lung dysfunctions like asthma or COPD? This is an area where our clinical experiences are at this point far outdistancing the available research.
One of the lung conditions associated with oxalate that has been studied quite a bit is sarcoidosis, which is a condition where granulomas are present. Granulomas are tumor-like masses of inflammatory tissue that consist of a collection of macrophages surrounded by lymphocytes and possibly giant cells. Giant cells are formed when multiple cells merge their membranes, forming one grand cell with multiple nuclei. Oxalate can induce that sort of merging of cells, and can also attract macrophages that can break down oxalate while turning on tumor necrosis factor. Another article we've listed below is a case study of someone with pulmonary hypertension caused by oxalates collecting in the blood vessels of the lung. Another patient developed amyloidosis in which oxalate was involved. A rat study found that oxalate given by IV left crystals in the lungs within an hour of exposure. Oxalate can also form in lungs after breathing in asbestos, but especially if someone has been taking ascorbic acid from which the oxalate could be derived.
Please look below for more information on current knowledge about the relationship of oxalate to the lungs.
Abstracts:
Bronchial Asthma, COPD in Combination with Hyperoxaluria
Clinical polymorphism in respiratory oxalosis
Wingate test performance in children with asthma: aerobic or anaerobic limitation?
The pathology of pulmonary sarcoidosis: update
Calcium oxalate and iron accumulation in sarcoidosis.
Acute oxalate nephropathy: A new etiology for acute renal failure following
nonrenal solid organ transplantation.
Hyperdense mucoid impaction in allergic bronchopulmonary aspergillosis: CT
appearance.
Oxalate deposition on asbestos bodies
Vitamin D toxicosis in cats: natural outbreak and experimental study
A case of oxalosis with heart and lung involvement
Subcutaneous deposition of beta 2-microglobulin amyloid in a long-term
haemodialysis patient
Calcium oxalate in sarcoid granulomas. With particular reference to the small
ovoid body and a note on the finding of dolomite
Significance of crystalline inclusions in lung granulomas
Excessive myocardial calcinosis in a chronic hemodialyzed patient
Multiorgan crystal deposition following intravenous oxalate infusion in rat
Electron microscopic detection of calcium ions at different stages of normal
surfactant formation and during body cooling
"Oxalate bodies", another reaction of the human lung to asbestos inhalation?
Localized endotracheal oxalosis probably secondary to aspiration of rhubarb
There is a very clear body of literature suggesting that those with cystic fibrosis, for various reasons, have increased risks of hyperabsorption of oxalate. (We have put a link to that literature below.) Several articles clearly advise the use of a low oxalate diet, but the truth seems to be, that in clinical practice, very few doctors give CF patients this advice.
Scientists do believe that the overexposure to antibiotics that is the usual treatment of CF coupled with the probems with poor fat digestion that happens in this condition comprise a formula for developing oxalate problems, but the literature doesn't reflect that research has looked at oxalate's consequences to other organs in CF besides the kidneys. Though those with CF do have increased risks of oxalate-related kidney disease, these problems are still not all that common in these patients as they get older. It is certainly possible, however, that oxalate that is hyperabsorbed all through life in CF may be causing or contributing to other systemic problems that appear more commonly in these patients.
We have had some listmates on Trying_Low_Oxalates who have CF and are exploring the use of the low oxalate diet, I think it is terribly important that they are seeing changes in the congestion of the lungs which is part and parcel of the serious problems in CF. This may be related to the lack of a normal interplay of the transporter that is defective in CF with the regulation of other transporters that could affect the movement of sulfate and oxalate across membranes all over the body, resulting in increased sulfation of certain molecules (which has been discovered in the literature as reported below) and possibly increased uptake of oxalate into cells. This mechanism would be of great interest since oxidative stress appears to be one of the most serious consequences of elevated oxalates and is seen as a greater problem in exacerbations of this genetic disease. If the increased sulfation is also a result of a change in the rate of activity of the sulfate transporters, this might also mean that more oxalate would travel to the same places, as sulfate and oxalate often share the use of the same transporters.
We commend the families on our list who are willing to pay attention to the medical literature and use a low oxalate diet. Our listmates with CF are discovering for themselves which parts of the norrmal problems that complicate life with CF might be caused by the involvement of excess oxalate in the disease process and may be preventable by this diet and other oxalate-reducing strategies.
We encourage those with CF to participate in our Trying Low Oxalates listserve especially because the cross-pollination with people with other oxalate-related conditions may help patients with CF recognize oxalate issues that they share with people with other conditions. We are excited that what they learn may give them information to share with non-CF listmates and with their doctors and with others they know with CF who may be eager to try this strategy for improved health.
Cystic fibrosis and oxalate
Is there a risk for kidney stone formation in cystic fibrosis?
Cystic fibrosis and calcium oxalate nephrolithiasis
Urinary excretion substances in patients with cystic fibrosis: risk of
urolithiasis?
Absence of Oxalobacter formigenes in cystic fibrosis patients: a risk factor for
hyperoxaluria
Oxalate and calcium excretion in cystic fibrosis
Metabolic risk factors for stone formation in patients with cystic fibrosis
Antibiotic treatment-induced tubular dysfunction as a risk factor for renal stone formation in cystic fibrosis
Acute regulation of the SLC26A3 congenital chloride diarrhoea anion exchanger
(DRA) expressed in Xenopus oocytes
Which factors account for renal stone formation in cystic fibrosis?
The association of nephrolithiasis with cystic fibrosis
Diagnostic and therapeutic approaches in patients with secondary hyperoxaluria
Absorptive hyperoxaluria leads to an increased risk for urolithiasis or
nephrocalcinosis in cystic fibrosis
Factors increasing the risk for stone formation in adult patients with cystic
fibrosis
Organ-specific over-sulfation of glycosaminoglycans and altered extracellular
matrix in a mouse model of cystic fibrosis
Metabolism of sulfated mucopolysaccharide in cultured fibroblasts from cystic
fibrosis patients
Enhanced channelling of sulphate through a rapidly exchangeable sulphate pool in
response to stimulated glycosaminoglycan synthesis in pancreatic epithelial
cells
Does deficiency of arylsulfatase B have a role in cystic fibrosis?
Endothelial activation and increased heparan sulfate expression in cystic
fibrosis
Oxidative stress in Cystic Fibrosis and with oxalates
Calcium oxalate stone disease: role of lipid peroxidation and antioxidants
Kidney Stones have long been recognized as a key problem that may develop when excess permeability in the gut or when a diet too rich in oxalates leads to excess absorption of oxalate that came from food. The concentration of oxalate in the urine is definitely an important risk factor for the formation of stones, but is definitely not the only risk factor. Some risks are genetic and have to do with the loss of sufficient numbers of certain protective molecules that keep stones from forming in the kidney. Some risks are easily reduced, such as correcting the dilution of the urine by drinking more water!
To understand issues that are specific to the kidney, please see the excellent sites listed below.
Why should people with kidney stones stay in dialogue with people with other oxalate-related issues? We have learned that it is NOT appropriate to think that kidney stones will become a problem BEFORE other problems with oxalate will occur in the rest of the body. There are conditions (comorbities) that represent other issues pushed by the same mechanism, but these problems will show up in other organ systems, but we may not realize they are oxalate-related.
By learning details of what reducing exposure to oxalate has changed in people with many other conditions, we will better be able to recognize areas outside the kidney that may improve general health while on the diet. That knowledge can be a tremendous incentive for staying on the diet!
"Enteric hyperoxaulria" is a term that identifies the gut as the primary source of oxalates that show up in urine in certain individuals. The additional risk for excess absorption happens when gut inflammation, steatorrhea (poor fat digestion or maldigestion) or a leaky gut allows oxalate to get past the intestinal barrier. More discussion of mechanisms that lead to a leaky gut can be found by reading: Mechanisms Behind the Leaky Gut.
Please visit the following sites for more insights specific to kidney stone disease:
A lecture from John Asplin of Litholink on kidney stones.
niddk.nih.gov
mayoclinic.com
emedicinehealth.com
nlm.nih.gov
medicinenet.com
wikipedia.org
For information on genetic causes of kidney stones:and other oxalate related disease, please see ohf.org.
To see how the supersaturation of the urine changes the shape of oxalate crystals: click here
The thyroid is the key organ of the body other than the kidney which is known to collect oxalates, resulting in compromised function.
Below are listed some articles that show how commonly crystals of oxalate are found in thyroid tissue. The concentration gets higher the older your age. The oxalate in the thyroid gland can render the patient hypothyroid, but elevations of oxalate may also be associated with developing auto-antibodies to the thyroid co-signalling molecule called p62. Scientists think the p62 level probably becomes elevated after exposure to oxalate because of membrane damage to cells. The autoantibodies against p62 that may develop in this situation are not only seen in thyroid disease but may also be seen in lupus or cirrhosis or connective tissue disease.
This nucleoporin, p62, is a factor involved in the signaling that we get from the active thyroid hormone T3, but it is also an oxalate binding protein. It is not entirely clear how it shares these two functions, but we should expect that antibodies to this factor coupled with elevations of oxalate may keep this molecule from providing the co-signal that makes T3 do its job in the nucleus of cells of all sorts. If this is happening, it may not matter how normal your thyroid levels in blood are, because a problem with the thyroid hormone signal in the nucleus may not be reflected as a change in blood level of T3 or T4 or TSH.
A lack of the T3 signal may be associated with Wilson's temperature syndrome, where people run a chronically low temperature that may respond to T3 medication given without T4. You can find information on the CLINICAL side of this issue at: Wilson's Syndrome , but there is some controversy in this area and some skepticism about the acceptability of claims made on this site by other thyroid experts. More research needs to be done, obviously. In the meantime, if you have a chronically low temperature that does not respond to T4, and possibly not to Armour thyroid which contains both T3 and T4, then your doctor may need to do some further lab work and decide whether it would be better to stick with giving you only T3 (Cytomel).
You may find your doctor got most of his information on thyroid problems from the people who make Synthroid, which is an artificial version of T4. In fact, he may not have heard that if the thyroid thinks it has too much T4, it will convert T4 into reverse T3 (rT3) rather than make more T3, which is the active hormone. Reverse T3 thyroid hormone actually inhibits the active thyroid hormone signal from T3 as apparently also does oxalate. That is why patients with any suspicion of oxalate problems and who plan to get their thyroid tested should make sure their doctor is acquainted with the literature on this area and get him or her to order a test of reverse T3 at the same time as the regular thyroid panel. Giving more T4 will not help increase thyroid activity if this medicine is being converted into reverse T3. Knowing to test for reverse T3 on your FIRST thyroid panel may save you months of doing trials with the wrong form of thyroid for you!
There also is a peripheral conversion of T4 to T3, but there is very little known about disorders related to peripheral conversion. A defect here may produce "thyroid issues" even when the usual thyroid panel comes out looking relatively normal. We need scientists to do more research in this area.
Please take a look at the articles below to get a deeper understanding of the connection of oxalates to the thyroid and to possible autoimmune issues.
The effect of dietary ingestion of oxalic acid on thyroid function in male and female Long-Evans rats
Calcium oxalate crystals in the thyroid. Their identification, prevalence,
origin, and possible significance
Birefringent (calcium oxalate) crystals in thyroid diseases. A
clinicopathological study with possible implications for differential diagnosis
Birefringent crystals in human thyroid
Nuclear pore complex oxalate binding protein p62: expression in different kidney disorders
Nucleoporin p62 antibodies in a case of mixed connective tissue disease
Family Thyroid Issues and Risks for Autism
Isolated nasopharyngeal aspergillosis caused by A flavus and associated with
oxalosis
Peripheral conversion of T4 to T3
Cold stress, reverse T3 and lymphocyte function
Effects of triiodothyronine supplements on splenic natural killer cells in malnourished weanling mice
Vulvodynia is a pain condition in women in the female area that can be quite disabling. More than a decade ago, the Vulvar Pain Foundation began a project under the direction of Dr. Clive Solomons who is an expert in connective tissue disorders. Their project explored the benefit of a low oxalate diet in solving this pain disorder. Not only has this strategy proved effective in many women, but it has also helped the same women resolve other health issues that might also have some link to oxalate. We are very thankful for their pioneering work in this area, and also grateful for the additional testing of foods for oxalates that they have done with Dr. Mike Liebman, producing the Low Oxalate Cookbook (Version 2). There is no reason to go into complete detail on their project here, since their website is so easy to access: Vulvar Pain Foundation.
The experience of these women is very valuable to us here, especially in broadening our understanding of what reducing oxalates may accomplish, so we do hope that those who find more specific support from the VP Foundation, will still actively participate here and enhance the cross-talk.
One major difference has appeared in the view of the low oxalate diet given by the VP Foundation and the view at lowoxalate.info. When the VP Foundation recognized that periodically those on the diet saw increases in oxalate in the urine along with increases in symptoms, they thought this might come from stepped up endogenous production, implying (to them) that perhaps the body was recognizing a deficiency of oxalate and trying to correct it.
As far as we have been able to determine, a purposeful production of excess oxalate has never been described in the literature in mammals. We do know that plants step up oxalate production in response to metal toxicity, and can store the oxalate bound to metal in specialized cells called idioblasts. The only time stepped up production has been recognized in humans is when a gene defect or vitamin deficiency leads to an excess of a precursor to oxalate that could be used by some other enzymes in the body to produce oxalate. The result in this situation has been toxicity.
Of course, with two different views of what MIGHT explain the periodic increase in urinary oxalate on a low oxalate diet, we are limited by the sorts of studies that have been imagined and conducted by the scientific community. Our project has the goal of enlisting new scientists to do the studies to make these distinctions as we get appropriate funding.
At the beginning of this oxalate project, we found what seemed a better explanation for these periods of increased oxalate in the genetic hyperoxaluria literature. This literature told us that oxalates will be taken up into tissues when there is too much circulating in blood, and there it will stay causing damage, Even so, it can be persuaded to leave those tissues when the concentration gradient of oxalate in the blood is lowered. That is what we expect happens during the diet if oxalate in the diet had been the continuing source of oxalate.
As our listmates noticed big improvements immediately following these presumed "high oxalate moments" that occurred when diet could not be the source of the oxalate, we decided that such a process of detoxification may reasonably become the point of the diet - to get the diet low enough to be able to observe oxalate leaving tissues and returning those tissues to normal function. Of course, even if the symptoms that needed treating are specific to one part of the body (like vulvodynia), detoxing from oxalate could involve oxalate leaving many other tissues all over the body where the effects might have been different from pain.
It is doubtful that oxalates leave tissues at a constant rate on LOD, for this process seems to be like a ratchet as each quick downtown leads to new progress as the downturn ends. Presumably, oxalate that is higher in some organ than in the interstitial fluids and blood, will begin to shift its direction from absorption into the cell to secretion to the outside of the cell and from there it can end up in blood or urine, or secreted to the lungs (perhaps) or the skin. This gradient may be reached suddenly in some tissue of the body. In vulvodynia, this sudden release of oxalate may get the vulvar area hurting again until excess oxalates have cleared all the places they were stored, so there is none left to release.
"Dumping", as we have called these moments, does not occur on a predictable schedule. That could mean, if a study were designed such as the one below that was done for vulvodynia, some portion of the the women in the study may have still been "dumping" at the final evaluation at the end of three months. We have seen that some who have been on LOD for two years still report that they have periods of "dumping". The medical literature tells us that it can take anywhere from several months to as long as four years for this detoxing process to be over after a liver transplant removed the source of excess oxalates in someone with primary hyperoxaluria. This keeps our eyes on long-term goals, and fortunately, the improvements (many that are surprising) are what keeps so many people motivated to continue until their healing is complete.
Pelvic disorders in women: chronic pelvic pain and vulvodynia
Vulvodynia associated with coeliac disease
Urinary oxalate excretion and its role in vulvar pain syndrome
Calcium citrate for vulvar vestibulitis. A case report
This information is protected by copyright laws, but may be used by individuals for their own use. Any publication of these materials outside this site may only be done after expressed permission from the authors. They may be contacted here....
Also, the information on this site must not be construed as medical advice. Any medicines mentioned on the site must be prescribed by a licensed professional. Please consult your own health care professional about how any information on this site could fit into your own or your child's health care regime.
{kind=link}